My post on June 24, 2025 was entitled, “I like Parkinson-like.” It was about a paper that was about to hit the stands (a Boomerism) authored by myself and Dr. Junaid Siddiqui of Cleveland Clinic. It proposed replacing the terms “atypical Parkinsonism,” “atypical Parkinsonian disorder” and “Parkinson-plus disorder” with a new term, “Parkinson-like disorder” (or “Parkinson’s disease-like disorder” because let’s not get TOO prescriptive).
The June blog post promised to make a copy of the paper available to you all once it was published. Better late (by seven months) than never. My mind was jogged by one of my current projects, preparing a lecture on the atypical Parkinsonian disorders in general that I will deliver at the University of Vermont in April. Also jogging my mind was that it’s been nearly two weeks since my last post.
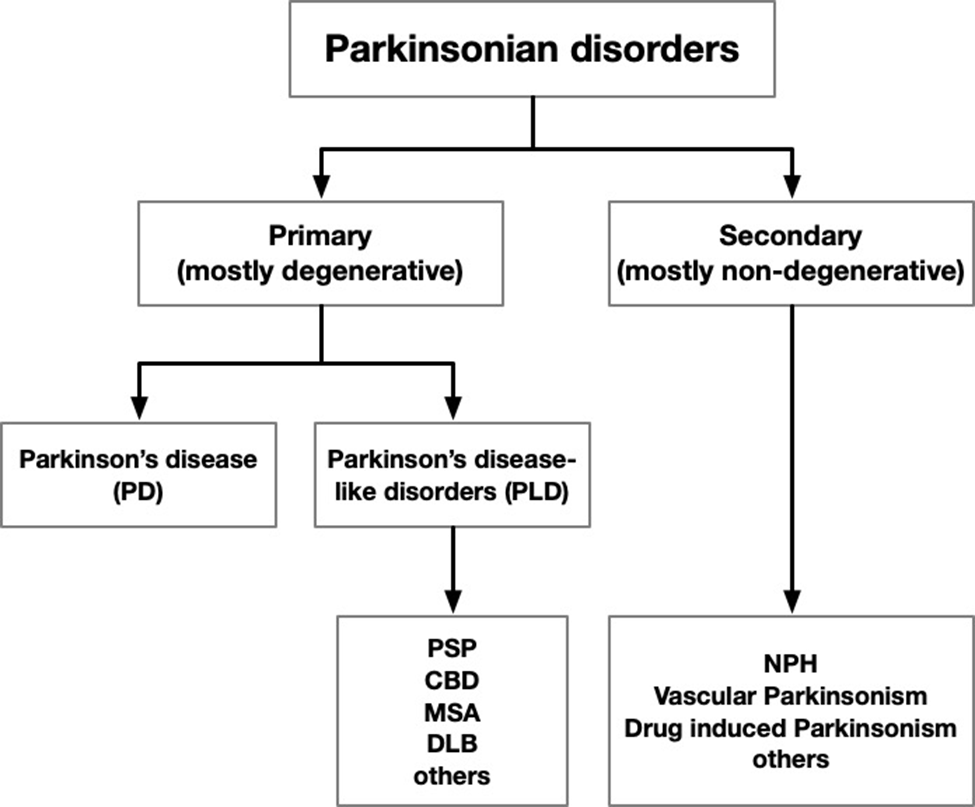
The pdf is at the bottom. If you have difficulty downloading or viewing it, here’s a link to the abstract and highlights and here’s a chart showing the gist of our proposed new terminology:
Does anyone like being called “atypical”? That adjective often conveys a foreign-ness or other-ness, and not in a good way. If you agree, you will be glad to know that a colleague, Dr. Junaid Siddiqui of the Cleveland Clinic, and I are about to publish an opinion piece entitled, “Time to Retire the Term “Atypical Parkinsonism.”
Over my career as a movement disorders subspecialist, I’ve heard both from professional colleagues and my patients that the term “atypical Parkinsonism” for PSP, CBD, MSA and a few other conditions is unwelcome. First, it implies that those conditions are simply unusual variants of Parkinson’s disease. However, they are actually independent diseases at the microscopical, molecular, and clinical levels with some features in common with PD. A similar problem applies to the term “Parkinson-plus.” PSP, CBD, and MSA aren’t simply PD with some additional features.
Yes, those three disease do include some degree of “Parkinsonism,” but that only means that they share a collection of outward slowness, muscle rigidity, impaired balance, and in some cases, tremor. Of course, the Parkinsonism of PSP, CBD, and MSA differ from that of PD. But that’s not because the first three are atypical versions of the fourth – it’s because they’re fundamentally different diseases.
That’s the scientific argument, but there’s also an emotional one. As I mentioned at the outset, no one wants their uncommon disorder to be considered an appendage of some other, more frequent one with superficial similarities. That would suggest that the uncommon condition is unworthy of its own approaches to support, treatment, and scientific study.
So, Dr. Siddiqui and I propose replacing the terms “atypical Parkinsonism,” “atypical Parkinsonian disorder,” and “Parkinson-plus disorder” with “Parkinson-like disorder.” This avoids the implication of inferiority and other-ness without losing the “Parkinson” term familiar to every physician.
The “-like” term has precedent in “Huntington-like disorder,” “polio-like syndrome,” and “stroke-like syndrome,” and that’s only in neurology. Yes, changing medical language can be a heavy lift, but it’s been done before. Examples just in movement disorders are Steele-Richardson-Olszewski syndrome to PSP, paralysis agitans to Parkinson’s disease, striatonigral degeneration to MSA-Parkinson, sporadic olivopontocerebellar ataxia to MSA-cerebellar, and corticodentatonigral degeneration to corticobasal degeneration.
Glossary of proposed terminology:
Existing
Proposed
Definition/comments
Parkinson’s disease
Parkinson’s disease
No change proposed
parkinsonism
Parkinsonism
A group of phenotypic features, not specific disease(s). The first letter should be upper-case.
Parkinsonisms
Parkinsonian disorder
Multiple members of a group of specific disorders featuring Parkinsonism
Primary parkinsonism
Primary Parkinsonian disorder
Any neurodegenerative disorder featuring Parkinsonism as a major component, at least in a majority of cases
Secondary parkinsonism
Secondary Parkinsonian disorder
Any non-degenerative disorder featuring Parkinsonism in at least some cases or at some point in the illness
Atypical Parkinsonism or typical Parkinsonian disorder
Parkinson-like disorder
Reserve “Parkinsonism” for a group of phenotypic features. Reserve “Parkinson-like” for specific diseases. Replace “Parkinson-plus” with “Parkinson-like disorder” as well.
Our paper will appear in the journal Parkinsonism and Related Disorders in a few days or weeks, at which time I’ll post you a link. Of course, if the journal itself follows our recommendation to confine the term “Parkinsonism” to a collection of signs and symptoms rather than allowing it to refer to specific diseases, then it will have to change its own name! But — as I always tell my students and patients, one step at a time.
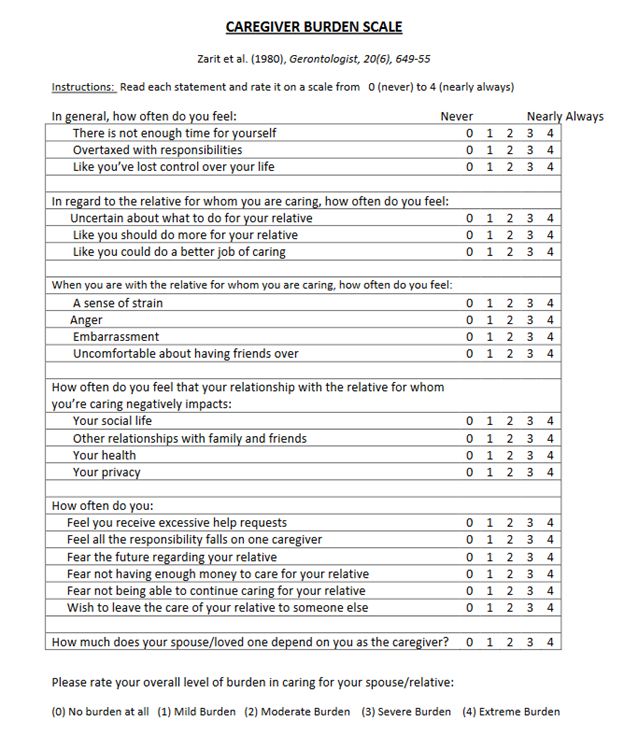
This audience does not have to be told that caring for a loved one with PSP can be a major burden. Two CurePSP Centers of Care have now quantified this using the Zarit Caregiver Burden Scale completed from 2014 to 2022 by 139 caregivers of 131 persons with atypical Parkinsonian disorders. The results are published in Clinical Parkinsonism & Related Disorders. Here’s the scale:
Ninety (65%) of the caregivers were women. Of the 131 patients they were caring for, 59% had PSP, 28% MSA and 13% CBS. The patients were on average about 4.5 years into their illnesses. (All three disorders have about the same average rate of progression and survival duration.) Here are the salient statistically significant results, adjusted for potential confounders as necessary:
The average (i.e., mean) total score was 28.8 of a possible 88.
Of the four disorders, PSP, CBS and MSA-cerebellar gave similar average scores, but scores for MSA-Parkinson were milder by a margin of about 8 points.
Female patients regardless of diagnosis involved a greater caregiver burden than males, regardless of the caregiver gender.
Female caregivers reported greater burden than males regardless of the patient’s gender or diagnosis.
The authors list several weaknesses of the analysis and propose a prospective study to avoid these. They include the absence of consideration of:
the relationship between patient and caregiver
age and any chronic illness of the caregivers
changes in the score over time
measures of the patient’s disability, especially falling frequency
The authors’ subjective opinion is that the patient’s cognitive and behavioral deficits are perhaps the most important determinant of the caregiver’s burden. A future study should examine this hypothesis in a formal way.
Adding these variables to the analysis would require a larger number of patient/caregiver pairs. This might be best accomplished in the context of a large treatment trial, where “secondary” and “exploratory” measures always accompany the “primary” measure of the drug’s efficacy. Alternatively, all 36 CurePSP Centers of Care could undertake such a project outside of any treatment trial, assuming adequate funding is available.
The first author of the new paper is Jessica Shurer, a medical social worker who serves as CurePSP’s Director of Clinical Affairs and Advocacy. The two senior authors are neurologists Alexander Pantelyat and Miriam Sklerov, directors of the Centers of Care at Johns Hopkins and the University of North Caroline at Chapel Hill, respectively, The three are credited with having conceptualized the study along with the second-named author, Margaret Ivancic, a medical social worker at UNC.