A support group leader in Florida just sent me his notes from a presentation by an occupational therapist. She made some sensible safety recommendations that I had not heard before, so I’m passing them along to you:
Increase the lumens of light bulbs around the house, especially in the bathroom, kitchen and stairways, three frequent locations for falls.
Despite the need for better light, glare from overhead lighting or a window can impair visual performance. So, use window treatments to diffuse direct sunlight, use shades on bare bulbs and consider multiple task lighting units in strategic locations instead of a single, bright fixture.
Use night lights controlled by a motion sensor. These are available with battery power, so that they can be placed anywhere.
If you don’t have carpet on your stairway, attach a tread with a reflective strip on each step and different-appearing ones on the top and bottom landings.
Some walkers are available with floor lighting.
To ease the task of locating food on the plate, use plates that contrast with that specific meal’s food.
Remove loose rugs from bathroom floors. To avoid slipping on wet spots, try stiff, rubber mats that stick to the floor.
Grab bars in and around the shower/tub and toilet are an obvious thing, but make sure they’re installed into studs.
Use grab bars with suction cups in temporary situations such as travel.
Toilet safety rails that rest on the floor allow safer landings onto the seat and easier liftoffs, especially if paired with a seat riser.
A bidet is a good idea if you have trouble wiping. Many models can be installed in a few minutes (according to the manufacturer) by someone with no plumbing skills.
Keep in mind that this is not a complete list – just a few things that I had not seen or written about before. Www.curepsp.org has lots more advice on optimizing daily activities, including pamphlets and videos.
I also hasten to add that no list of tips is a substitute for a consultation with an occupational therapist with follow-ups as your symptoms evolve over time. If you can’t find one and your doctor doesn’t know one, just call the OT department in your nearest good hospital for recommendations.
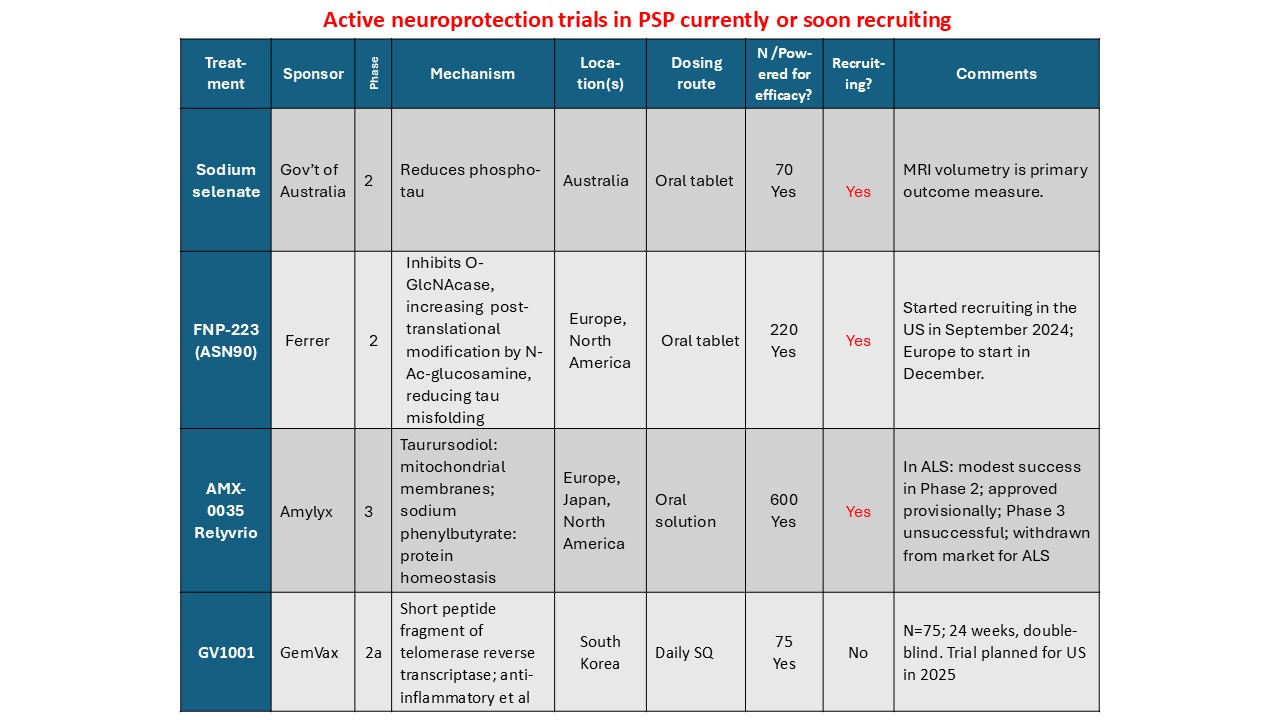
It’s high time I updated you on currently – or imminently – recruiting PSP clinical trials.
Here are the four in chronological order. All these are for “neuroprotection,” meaning slowing of the underlying disease process. They don’t attempt to improve the existing symptoms, however. That’s called “symptomatic” treatment and I’ll get around to that soon.
More details:
Sodium selenate provides supplemental selenium, which is critical for the function of 25 human enzymes with a wide range of functions. Two are relevant to PSP: glutathione peroxidase 4 and protein phosphatase 2A. The first regulates one type of programmed cell death and the second removes phosphate groups abnormally attached to the tau protein. The trial is happening only in Australia. See here for details, including contact information.
FNP-223 inhibits an enzyme called 0-GlcNAcase (pronounced “oh-GLIK-nuh-kaze”), which removes an unusual sugar molecule from its attachment to tau. The sugar is called N-acetyl-glucosamine and it prevents abnormal tau from attaching at the same spots on the tau molecule. It’s an oral tablet and the trial, which has just started, will be in both Europe and North America. Click here for details and contact info.
AMX-0035 is a mixture of two drugs in an oral solution. Both are currently marketed for conditions unrelated to neurodegeneration. The PSP trial has started in North America and will do so in Europe and probably Japan in the next few months. One of the two drugs, called sodium phenylbutyrate (marked as Buphenyl), addresses the brain cells’ management of abnormal proteins. The other, taurursodeoxycholic acid, marketed as TUDCA, helps maintain the mitochondria. Click here for details and contact info.
Finally, GV-1001 is an enzyme with anti-inflammatory action in the brain. But it’s not like a steroid or non-steroidal anti-inflammatory drug. It acts by an mechanism that the drug company is keeping close to its chest and has something to do with DNA transcription into proteins. The drug has to be injected subcutaneously every day, like insulin. A small trial is in progress in South Korea and in you live there, here’s enrollment info. There are plans to start a trial in the US in 2025, but that could depend on the current trial’s outcome.
Soon, I’ll post something on neuroprotection trials in which the double-blind recruitment is over but the results are pending. After that will be symptomatic trials.
With all these trials in progress, CurePSP’s “Hope Matters” tagline is truer than ever.
I’ve not posted much in a while. Lots of other commitments, but unlike this blog, they had deadlines, you see. So, I have lots to catch you up on, starting with a cool study in zebrafish. This cute, 1-2-inch fishy is a popular aquarium pet. As it turns out, it also makes a great animal model for PSP.
The model is created by injecting a normal human tau gene into a fertilized fish ovum. Human tau comes in six different versions, called isoforms. The tau gene used here encodes only the single isoform that accumulates in the neurofibrillary tangles of typical, non-hereditary PSP, called 0N4R tau. The resulting adult fish not only swims poorly — its eyes don’t move very well, either. It can then be bred to form an ongoing colony. Compared with mice, the leading PSP model until now, zebrafish are cheaper and easier to maintain and provide a much more efficient way to screen dozens of drugs quickly.
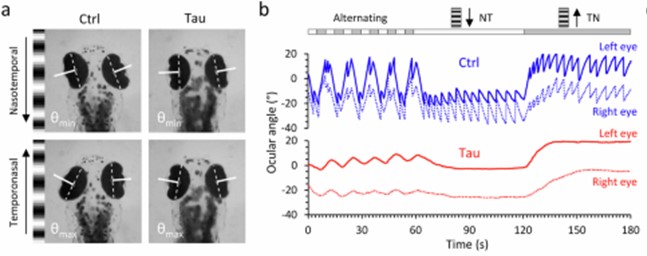
The figures below are from a new publication from the University of Pittsburgh led by senior author Dr. Edward A. Burton with first author Dr. Qing Bai.
Panel A shows still images from a video of a zebrafish as seen from above. The large, dark ovals are eyes and the smudge toward the bottom is the body. Panel B shows the movements of the eyes when shown a moving array of black-and-white stripes. The blue tracing is from a fish without the added human tau gene. Its eyes move crisply from one stripe to the next, but the red tracing, from a fish with the human tau gene, shows a weak response. This is identical to the response in people with PSP who are asked by a neurologist to count the stripes on a strip of cloth moved across their field of vision. It’s called “opticokinetic nystagmus” and is a good way to detect the earliest, asymptomatic involvement of the eye movements of PSP or some other disorders.
If you go to the link provided above and scroll down to the link for “Supplementary movie 1,” you’ll see a video of the eye movements and the stimulus stripes.
Armed with this experimental set-up and another to trace traced the fish’s spontaneous swimming in a circular dish, Drs. Bai and colleagues then screened a panel of 147 chemical compounds for any ability to correct the problems. The 147 were chosen because of their ability to modulate the attachment of small molecules to genes, one type of “epigenetic” alteration that we know occurs in PSP. Large drug screens in vertebrates are much more easily performed in zebrafish than in mice.
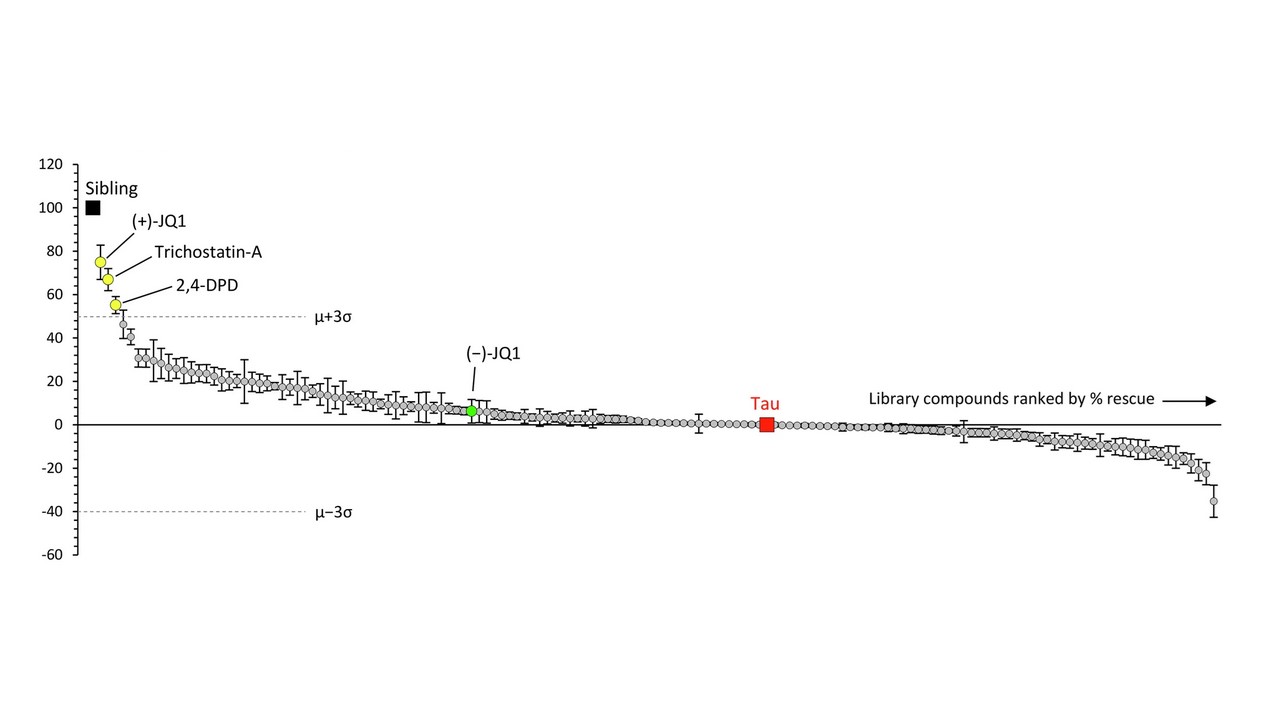
The graph below shows the results. Each circle is one drug and the vertical axis is the improvement or worsening it produces in the zebrafish. The “whiskers” on each circle indicate the variation among the 12 fish tested on that drug. The drugs’ results are displayed left-to-right in descending order of benefit, which means that the drugs on the right, below the “0” line, were actually deleterious. The black square labeled “sibling” indicates a littermate fish without the human tau against which the drugs’ effects are compared. The red square labeled “tau” shows another kind of comparators — the fish with human tau that were left untreated. The dotted, horizontal lines are placed at a point three standard deviations (σ) from the average (μ) of the 147 drugs’ degree of benefit (upper line) or worsening (lower line). That’s the researchers’ threshold of significant interest for the drugs.
The best-performing drug was something with the weird name, (+)-JQ1. It’s a member of a group called “bromodomain inhibitors,” which have nothing to do with the element bromine. A bromodomain is a string of 110 amino acids that forms part of many proteins involved in regulating the transcription of certain genes into their own proteins. Other inhibitors of bromodomain-containing proteins are being tested as treatment for various cancers. My clinicaltrial.gov search on “bromodomain inhibitor” produced 52 such trials, though none so far for (+)-JQ1 itself. The second-best bromotomain inhibitor emerging from the zebrafish screen is trichostatin-A, a non-FDA-approved, anti-fungal antibiotic with potential anti-cancer properties and 137 listings in clinicaltrials.gov. Third is 2,4-OPD, on which I found no information anywhere.
Bonus fact for the real science nerds: The graph shows a green data point for (-)-JQ1. That’s the “enantiomer” of (+)-JQ1. Enantiomers are pairs of molecules with identical sets of atoms in mirror-image configurations. Some such pairs have identical properties but many don’t. A good example of the latter is levodopa, the (-) version of dihydroxyphenylalanine. It helps Parkinson’s dramatically and PSP modestly, but the (+) version, which would be called “dextrodopa,” does neither. The “dextro-” and “levo-” prefixes refer to the clockwise or counterclockwise rotation that a solution of the compound imparts to the plane of polarized light.
So, let’s await experiments of (+)-JQ1 and trichostatin-A in other models such as tau knock-in mice, stem cells and organoids. Let’s also await screens of other classes of drugs in the cute little zebrafish that provide a great new, efficient test bed for PSP treatments.