My post from two weeks ago, entitled, “A big little fish,” was about zebrafish as an experimental model for PSP. This creature, once the normal human tau gene has been added to its genome, is uniquely suited for efficiently screening long lists of drugs as treatment for tauopathies. I specifically cited a publication screening 147 currently available drugs modulating the attachment of phosphate groups or other regulators of tau production. It yielded two reasonable candidates for further research in other animal models or in people with PSP.
This week, there’s another important finding in zebrafish, except that it concerns not tau production, but tau disposal.
A research group at the University of Cambridge led by Drs. Ana Lopez, Angeleen Fleming and David Rubinsztein used zebrafish with the normal human tau gene to screen 1,437 compounds for use against tauopathies. All had been either FDA-approved for medical use or found in clinical trials to be safe, even if ineffective for whatever they were being tested for.
Next, they tested those 1,437 for the ability to improve the survival of a set of cells in the fishes’ eyes (the rods) that normally produce the tau protein. Of the 71 passing that test, the researchers chose the 16 that seemed easiest to study further. Of those, the most effective at rescuing cells from degenerating was the drug methocarbamol, which is available by prescription for muscle spasms under the brand name “Robaxin.” One of the several actions of methocarbamol unrelated to muscle relaxation is inhibition of an enzyme called carbonic anhydrase, which regulates the acid-base balance of cells.
Drugs that specifically inhibit carbonic anhydrase are available for use in glaucoma and in a variety of neurological disorders. Three of the most popular anhydrase inhibitors are acetazolamide (brand name Diamox), methazolamide (Neptazane) and dorzolamide (Trusopt). To determine if carbonic anhydrase inhibition explains the benefit of methocarbamol in the zebrafish, the researchers gave those three drugs to a different colony of zebrafish with a human tau gene, but in this case the human gene carried a mutation called P301L, which causes a rare, hereditary, PSP-like illness.
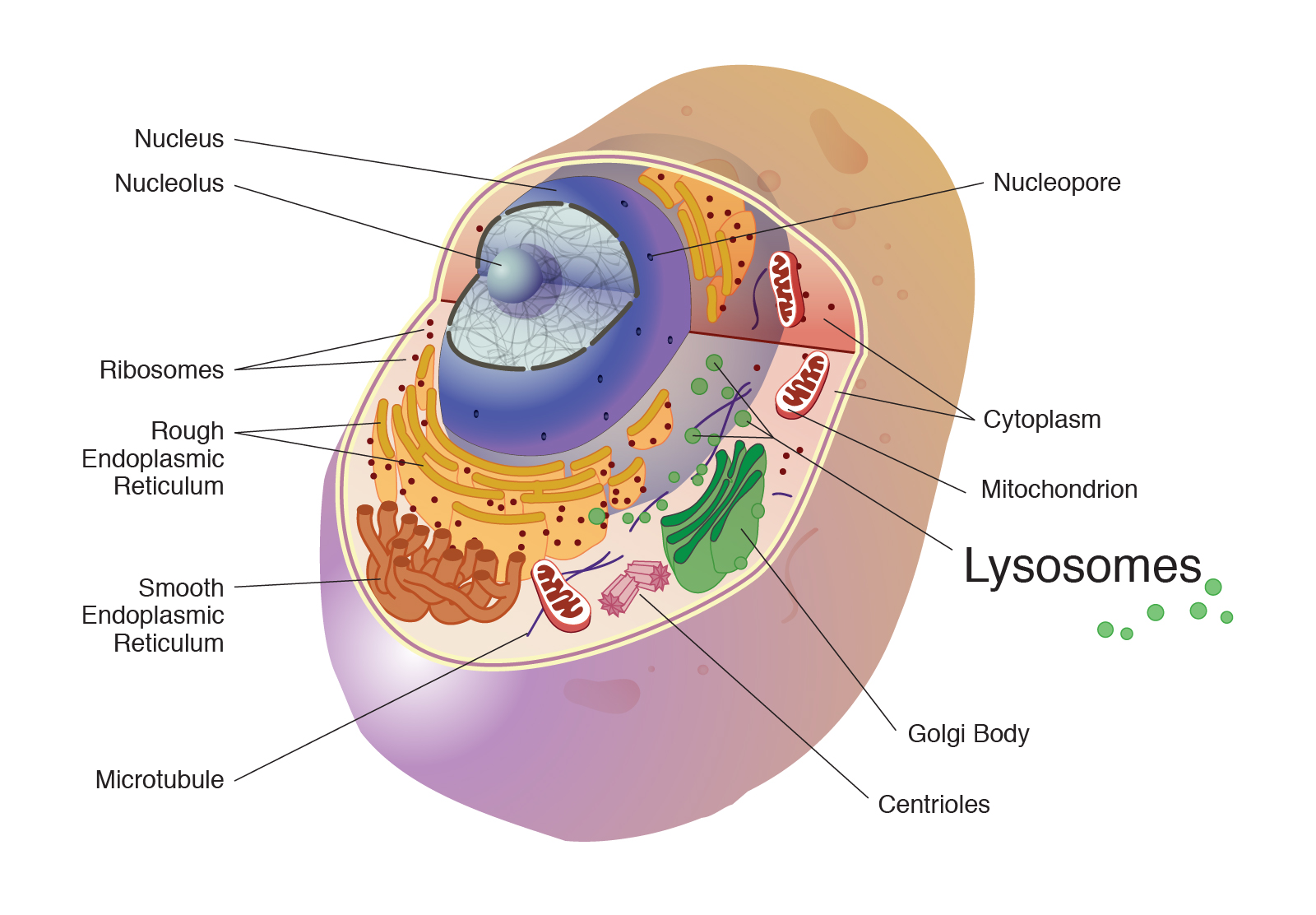
To the Cambridge team’s delight and ours, all three carbonic anhydrase inhibitors provided major protection against the damage caused by that tau gene mutation. A further set of experiments showed that the mechanism of protection was that the drugs work by improving the export of tau from the cells by the lysosomes. Those are organelles that perform part of our cells’ complicated garbage disposal mechanism.
I’ll let the researchers’ own words describe the overall results:
Together, our results suggest that CA [carbonic anhydrase] inhibition ultimately regulates lysosomal acidification and cellular distribution, promoting lysosomal exocytosis and tau secretion. This mechanism lowers tau levels within neurons, which, in turn, have lower levels of hyperphosphorylated and aggregated toxic tau forms, accounting for an improvement in phenotypic, neuronal loss and behavioral defects in vivo in zebrafish and mouse models. This raises the possibility of rapid repurposing of CA inhibitors for tauopathies, as our studies were performed in mice at human-like plasma concentrations. Furthermore, our data suggest that stimulation of unconventional secretion may also be a potent therapeutic approach for other neurodegenerative diseases caused by toxic, aggregate-prone intracellular proteins.
So, the “elevator explanation” is that carbonic anhydrase inhibitors make the fluid in lysosomes more acidic, enhancing their ability to load up on abnormal tau protein and dump it out of the brain cell.
This finding could lead to repurposing existing, off-patent carbonic anhydrase inhibitor drugs not only for PSP but potentially also for the many other neurodegenerative diseases that rely on the lysosomes to dispose of abnormal, misfolded proteins. Let’s hope that other animal models confirm this and that a clinical trial follows.
All the carbonic anhydrase inhibitors available are off patent, which means that their manufacturers would not be interested in investing the many millions of dollars needed to test them for a new use. But drug companies have been known to reformulate old drugs into longer-acting or better-absorbed versions, or to make inconsequential but patentable tweaks to old drugs’ chemical structure. Or maybe a deep-pocketed, non-commercial funder such as the NIH could fund a clinical trial of an existing carbonic anhydrase inhibitor.
So, that’s what should happen . . . and here’s what should not happen: For you to doctor-shop until you find one willing to prescribe a carbonic anhydrase inhibitor. For one thing, those drugs come with a long list of possible side effects and drug interactions. For another, it would be difficult to know if it’s working to slow the rate progression in you as an individual. If you go on a potentially neuroprotective drug and develop some moderate side effect, the decision to continue or discontinue the drug would depend on its benefit in you specifically, not on its effect in zebrafish or even in other people with PSP averaged together. That’s why drug trials observe each participant for a whole year and involve hundreds of participants randomized to experimental drug or placebo. We need faster and cheaper ways to do such trials and a lot of work is addressing that problem right now.
Meanwhile, don’t give up hope — or give in to the temptation of unproven, unmeasurable treatment.
