My post on June 24, 2025 was entitled, “I like Parkinson-like.” It was about a paper that was about to hit the stands (a Boomerism) authored by myself and Dr. Junaid Siddiqui of Cleveland Clinic. It proposed replacing the terms “atypical Parkinsonism,” “atypical Parkinsonian disorder” and “Parkinson-plus disorder” with a new term, “Parkinson-like disorder” (or “Parkinson’s disease-like disorder” because let’s not get TOO prescriptive).
The June blog post promised to make a copy of the paper available to you all once it was published. Better late (by seven months) than never. My mind was jogged by one of my current projects, preparing a lecture on the atypical Parkinsonian disorders in general that I will deliver at the University of Vermont in April. Also jogging my mind was that it’s been nearly two weeks since my last post.
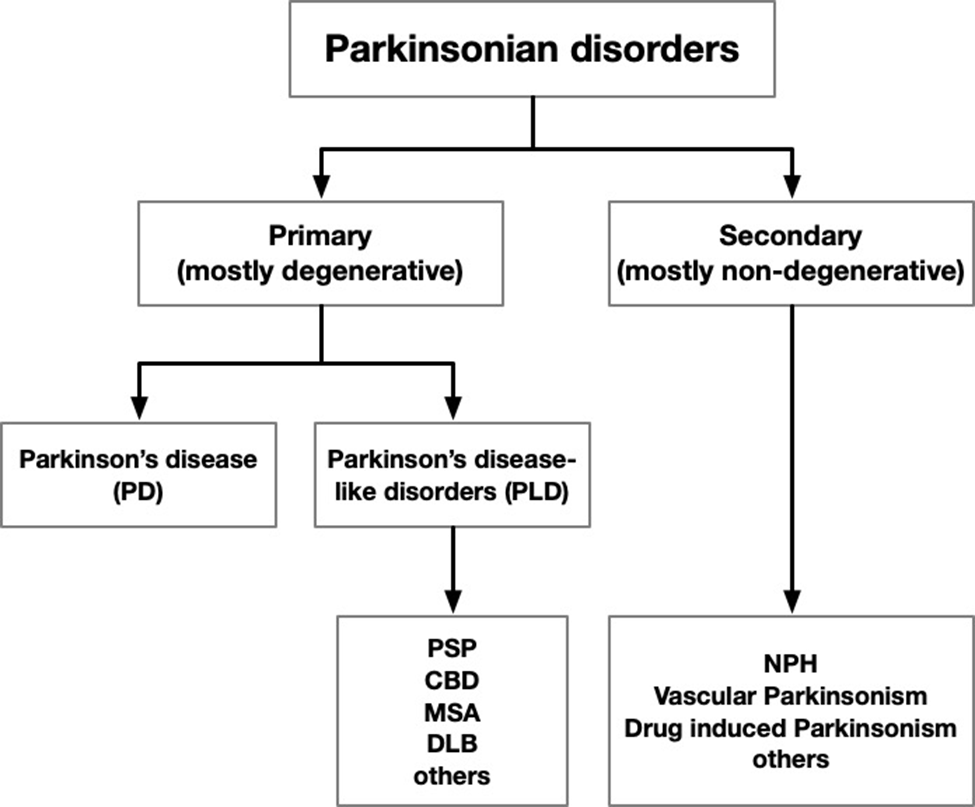
The pdf is at the bottom. If you have difficulty downloading or viewing it, here’s a link to the abstract and highlights and here’s a chart showing the gist of our proposed new terminology:
Yesterday’s post was about how the 10 most-frequently-visited news items in Parkinson’s News Today (PNT) of 2025 might relate to PSP. The list appeared here.
#5: FDA clears early trial of stem cell therapy for Parkinson’s
The treatment, called XS-411, is made from stem cells derived from multiple healthy donors and converted into dopamine-producing cells. Each patient would receive one injection of such cells into each side of the putamen, the brain area where the dopamine synapses are located. The FDA approved a Phase I trial in April 2025, but now, nine months later, clinicaltrials.gov lists two small studies in China but none in the US. Most current stem cell trials in neurology derive the cells from the patient’s own bone marrow or skin biopsy, so I really don’t know why the company, XellSmart Bop-Pharmaceutical Company of Suzhow, China, is using cells from people other than the patients themselves. Maybe they have a new way to suppress the immunologic rejection or maybe production using multiple donors is more easily scalable to serve large numbers of patients. Could XS-411 work in PSP? Perhaps it could help the same fraction who respond to levodopa, which is only a minority, and their benefit is usually modest and transient. The problem is that in PSP, unlike in PD, the cells in the putamen receiving the dopamine-encoded signals are degenerating along with the dopamine-producing cells. So, we need more research into injecting stem cells producing neuroprotective molecules or non-dopamine neurotransmitters.
#4: Program offers psychedelics as treatment for Parkinson’s
Ibogaine is a psychedelic drug legal only in a few states, and even then only for FDA-approved research use. Ambio is a company offering the drug to people with a wide variety of conditions on a “research” basis at clinics in Mexico and Malta. There’s no such listing in clinicaltrials.gov, so I can’t be sure of the protocol except that patients are charged $6,050 for a four-day treatment initiation at one of their clinics and “micro-doses” for the next six months. Based on the little information available, this fits the profile of many “research trials” of alternative treatments: a hefty fee, minimal pre-treatment evaluation or followup, no control group and no peer-reviewed publication. In this case, I must also wonder about the risk of habituation to the treatment itself, and where do you suppose you could buy something to satisfy that? Enough – you now know what I think about this drug for PSP, even if the initial $6,050 and the travel expenses are not an issue for you. To be sure, some alternative treatments do have legitimate potential, but when there’s a major risk of financial or medical harm (both of which apply here), their use should be confined to formal FDA-approved research protocols.
#3: Bacteria in digestive tract tied to cognitive decline
Parkinson’s disease is a natural candidate for causation by intestinal bacteria because the first stage of the disease, aggregates of the alpha-synuclein protein in neurons, starts not in the brain, but in the intestines and lungs. But PSP does appear to start in the brain. There’s been little research on gut bacteria and PSP, but something important was reported in 2023 from researchers in China and summarized in my 4/2/23 post. That short-term study found that replacing the colonic bacteria produced about a 10 percent benefit in the PSP Rating Scale score. The trial was too short and small to conclude anything about long-term slowing of progression. Bottom line: Although PSP does not start in the GI tract as PD does, gut bacteria may play a role and should be studied further for any therapeutic implications.
#2: Study identifies potential way to treat Parkinson’s constipation
Ghrelin is a string of 28 amino acids with many basic gastrointestinal functions including stimulating appetite at the level of the brain and defecation at the level of the spinal cord. The article reported by PNT teased out an important detail that could hold implications for treatment of constipation in those with PD. We don’t know if applies as well to the constipation of PSP, but I can say that some of PSP’s constipation is caused by degeneration of a cluster of cells in the lower spinal cord that are not involved in PD. One research study, from 2013, did find a role of ghrelin in multiple system atrophy but not in PSP or corticobasal syndrome. So, those few strands of evidence suggest that people with PSP will have to rely on traditional methods of keeping things moving – exercise, fluids, fiber, a stool softener, and avoidance of drugs that block acetylcholine synapses (“anticholinergics”). Many drugs in the last category are used for other PSP symptoms such as imbalance, vertigo, urinary incontinence and depression, so getting off those is a good topic for discussion at the neurologist’s office.
#1: Research shows disrupted mitochondrial DNA tied to inflammation
For decades, we’ve known that in both PD and PSP, the cells’ mitochondria malfunction and there’s excessive inflammation in the brain. But we don’t know which is cause and which is effect, or if they’re both effects of a common cause. The new study used a novel genetic technique to find evidence that it’s the inflammation causing the mitochondrial loss. In theory, the same study could be performed in PSP. A similar result would suggest that to slow PSP progression, targeting excessive inflammation might do better than those targeting mitochondria directly. Early in my career, I had narrowed my subspecialty choices down to movement disorders and neuroimmunology/multiple sclerosis. I chose the former because I was flummoxed by the complexity of the immune system. Little did I know . . .
A couple of weeks ago I posted my curated list of the top 10 PSP-related research developments of 2025. They appeared in two installments on 12/31/25 (#1-5)
Clearly inspired by my effort, the publication “Parkinson’s News Today” (PNT) has done something similar for Parkinson’s disease, summarizing their 10 most-often-visited (not necessarily the most important) news stories of 2025. Their article is very well supplemented with links to both basic explanations and to the PNT articles themselves. Those PNT items link, in turn, to original journal articles and to press releases from drug companies or research institutions.
PNT is owned by a for-profit medical communications company and its on-line publication is monetized by advertising, mostly from drug companies. So be aware that their choice of what’s important may be biased in favor of drug companies’ products and scientific narratives. No such concrete instances have hit me over the head, but the potential for a conflict of interest is there.
Armed with that caveat emptor, you can learn a lot from this list, which is numbered from least to most important. Here are my annotations for each item, pointing out the relevance, or lack thereof, for PSP:
#10: Virus long thought harmless may trigger Parkinson’s
The brain tissue in PSP looks very similar to that of “post-encephalitic Parkinsonism” (PEP), which was quite common from the 1920s to 1950s. Both feature tau-based neurofibrillary tangles and attack the basal ganglia, but PEP is static over decades. It appears to be a immunologically-based , residual effect of a brain infection called “von Economo’s encephalitis” or “encephalitis lethargica.” The virus itself has never been isolated or identified. The disease overlapped, but is different from, the great flu pandemic following World War I. Otherwise, despite ample search, there’s little to no evidence that any virus can cause PSP.
#9: Scientists develop weekly injectable implant for Parkinson’s treatment
The implant (actually a viscous, intra-muscular, self-injected liquid) provides levodopa/carbidopa (LD/CD) for a week. Unfortunately, most people with PSP respond little or not at all to levodopa/carbidopa. However, in those with the PSP-Parkinsonism subtype and few with other subtypes, there can be a useful response for a few months of daily dosing. While those with PSP who do respond don’t need a long-acting form, avoiding having to take pills could be a major advantage for those with swallowing difficulty.
#8: DBS plus exercising may rewire Parkinson’s brain
The brain, even in older persons, can route its circuits around areas of damage, especially if those circuits are used often. That’s called “exercise” or “physical/occupational therapy” or just “practice,” (note my sarcasm) and it does work. This is true in PSP as well as in PD. But deep brain stimulation (DBS), at least the kind used in PD, does not work in PSP. That’s because the brain areas that are overactive in PD simmer down in response to DBS. But in PSP, those areas are part of the degenerative process itself, and are underactive. But to repeat: Informal physical activity and formal physical/occupational therapy do work in PSP. They should be an important part of the daily routine, assuming that one’s physician decides that any balance problems, osteoporosis, or cardio-pulmonary disorders are not contraindications.
#7: FDA approves bilateral Exablate Neuro treatment for Parkinson’s
Exablate is the brand name for a device that focuses destructive ultrasound beams on those over-active brain areas of PD. (It usually appears in the literature as “focused ultrasound” or FUS.) So, the idea is same as DBS, but FUS produces a permanent lesion that can’t be adjusted by the doctor based on the patient’s response. But its advantage of FUS over DBS is no hardware in the head, wires under the skin, pacemaker device in the chest, periodic battery changes, or explanations at metal detectors. Unfortunately, the FUS lesion locations used in PD would not work in PSP, but novel lesion locations could, in principle, be discovered for PSP for problems like balance, speech or cognition.
#6: Dosing starts in trial of anti-inflammatory therapy for Parkinson’s
PNT’s news item reporting the start of this single-center, Phase I trial appeared in March, as their blurb states, but I’ve got an update for you. The drug’s safety and tolerability were satisfactory but trial, with only 30 patient and one month’s observation, was not powered to demonstrate efficacy. The sponsor company, Ventus Therapeutics, has now started a Phase II trial for PD at 23 US sites. The drug, called VENT-02, targets NLRP3, a receptor protein activated by stress signals in the microglia, the brain’s equivalent of white blood cells. That could be relevant to PSP, where microglia help spread the abnormal tau protein through the brain and otherwise mediate the brain inflammation of PSP.
I’ll cover items #5 through #1 tomorrow or whenever my week’s chores permit.
Two terms used in the article that are probably not familiar to you in this context are “spasticity” and “apraxia.”
Spastic speech has a “rubber-band” quality, with abrupt variations in speed and loudness. It’s very common in PSP. It corresponds to spastic limb movements (rare in PSP), where joints can suddenly flex or extend in response to gentle movement or sensory input.
Apraxic speech features reduced ability to make certain sounds or words without a corresponding inability to form their components. It’s common in some of the APDs, but not in PSP. It corresponds to limb apraxia (common in PSP), where power and simple tasks are preserved, while more complex, learned tasks are impaired.
The paper includes videos of people with some of the APDs performing a standardized series of speech tasks, including describing the picture below:
The famous “cookie theft scene” test is designed to assess perception, judgement and language, but it serves as a test of voice and speech as well.
That brings us to the differences among “voice,” “speech” and “language.”
Voice difficulties include things like hoarseness and low/high volume.
Speech difficulties include things like slurring, slowing/speeding and disordered rhythm of sentences.
Language problems include things like wordfinding problems, word substitutions and reduced grammatical ability. It’s not discussed in the current paper but may be the topic of a subsequent review by the same group of neurologists.
A quick-and-easy way to organize this scheme is to consider voice problems as arising from the lungs and larynx; speech problems from the mouth, tongue and lips; and language problems from the brain.
The paper’s authors are all at institutions within CurePSP’s Centers of Care network. The leader of the project was Dr. Federico Rodriguez-Porcel of the Medical University of South Carolina. The other 25 authors, including yours truly, are listed in alphabetical order. So, as a clearly biased contributor, I recommend this paper on voice and speech in the APDs to those interested in understanding the range of such problems and their potential for rehabilitation.
Yesterday’s post was the first five of my top ten PSP news items of 2025. Here are the rest, again in approximate and subjective descending order of importance.
New ways of interpreting standard MRI images have gained ground as diagnostic markers for PSP. One is a test of iron content in brain cells called “quantitative susceptibility mapping” (QSM). Nine papers on that topic appeared in 2025, four in 2024 and none previously. It’s looking like combining QSM data from ordinary measurements of atrophy of PSP-related brain regions could be the ticket, as both measures come from the same test procedure, unpleasant though it may be, and they measure different things.
Positron emission tomography (PET) imaging of PSP’s type of tau (“4-repeat tau”) has made advances in 2025. This test requires intravenous injection of a “tracer” with a radioactive component that enters the brain tissue,sticks to the target molecule and is then imaged. It can distinguish PSP from non-PSP, distinguish among various PSP subtypes, and quantify the disease progression. The leading such tracer in terms of readiness for submission to the FDA is [18F]PI2620 and a distant second is [18F]APN-1607 ([18F]-PM-PBB3; Florzolotau). A tau PET tracer called Flortaucipir is on the market as a test for Alzheimer’s disease, but it performs poorly for PSP.
There’s brain inflammation in PSP, but it’s not clear whether it’s a cause or a result of the loss of brain cells, or both. Regardless, measuring the quantity and type of inflammation using blood or PET could shed light on the cause of the disease, identify new drug targets, and serve as a diagnostic marker. A good example of 2025 research on blood markers of inflammation in PSP is here and on PET imaging of inflammation is here .
We know of variants in 21 different genes, and counting, each of which subtly influences the risk of developing PSP or its age of onset. The area of the genome most important to PSP is the one that includes the gene encoding tau (called “MAPT”) on chromosome 17. The most important PSP genetic advance in 2025 was probably the discovery that some PSP risk is conferred by extra copies of a stretch of DNA, not the sequence itself. This news could inspire investigation of other places in the genome for other copy-number variants, which are much trickier to find than sequence variants. Here’s a great review of the latest in PSP genetics.
And lastly, a disappointment: a negative result of a double-blind trial of the combination of two drugs already approved for other conditions: sodium phenylbutyrate (“Buphenyl”) and taurursodeoxycholic acid (“TUDCA”). Blog post here.Sponsor’s press release here. Buphenyl protects the endoplasmic reticulum, which helps manufacture proteins, and TUDCA helps prevent brain cells from undergoing self-destruction (“apoptosis”) in response to various kinds of stressors. The pair were theorized to act synergistically. The trial’s upside is that its placebo group data can be used to provide better statistical support for future innovations in clinical trial design.